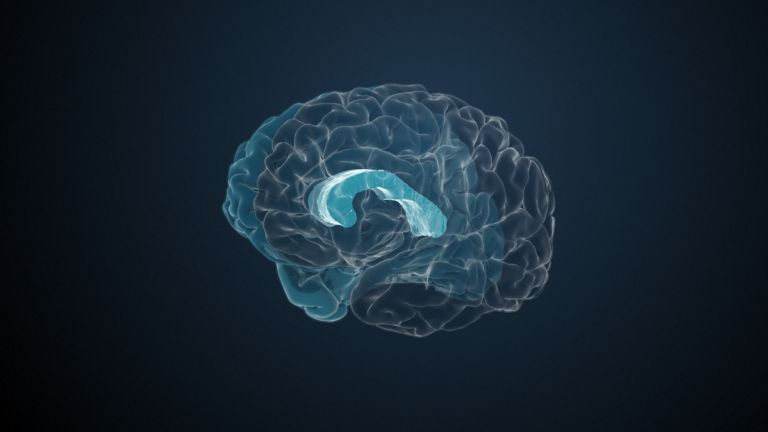
The Parietal Lobe

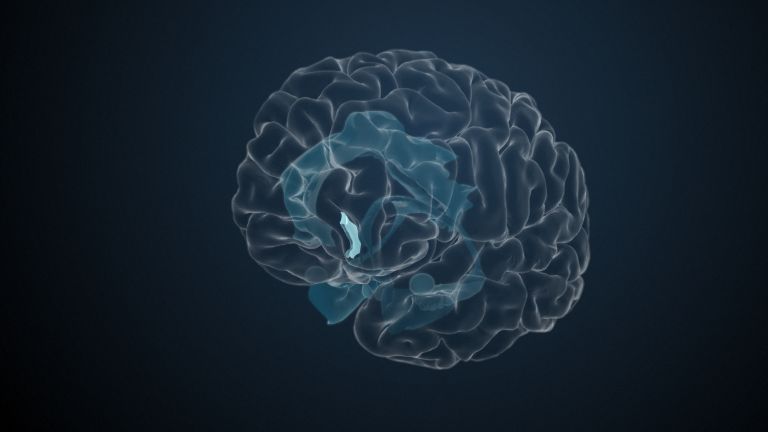
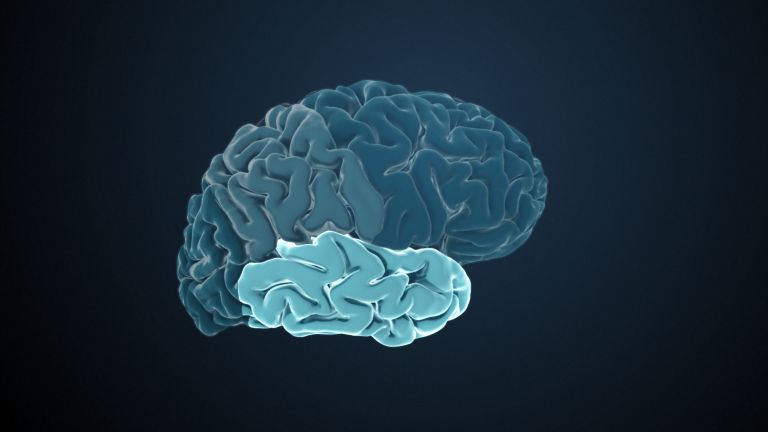
The parietal lobe is located behind the frontal lobe and is separated from it by the central sulcus. Two important nerve pathways that transmit bodily sensations such as pain, temperature, and touch end in the parietal lobe. However, the functions of the parietal lobe extend far beyond the body.
Scientific support: Prof. Dr. Herbert Schwegler, Prof. Dr. Anne Albrecht
Published: 18.09.2025
Difficulty: intermediate
The main function of the Parietal lobe is to process information from our somatosensory Perception: what does the body feel (e.g., touch, pain, temperature), and where and in what position are our own limbs? While this takes place in the somatosensory cortex, the rear area of the parietal lobe relates this information to the near and distant environment. Damage to these areas can lead to what is known as Neglect – to difficulties recognizing one's own limbs or one half of the environment.
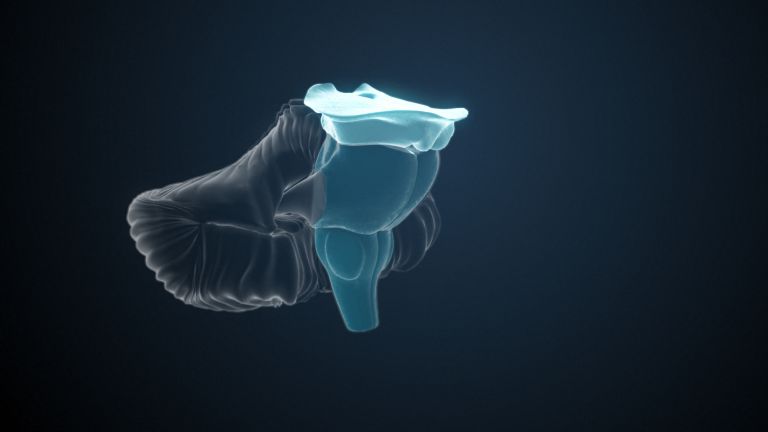
Parietal lobe
Lobus parietalis
The parietal lobe is one of the four large lobes of the cerebral cortex. It is located behind the frontal lobe and above the occipital lobe. Somatosensory processes take place in its anterior region, while sensory information is integrated in its posterior region, enabling the handling of objects and spatial orientation. In addition, the parietal lobe is involved in attention, the recognition of body parts and objects, as well as linguistic and mathematical abilities.
Perception
The term describes the complex process of gathering and processing information from stimuli in the environment and from the internal states of a living being. The brain combines the information, which is perceived partly consciously and partly unconsciously, into a subjectively meaningful overall impression. If the data it receives from the sensory organs is insufficient for this, it supplements it with empirical values. This can lead to misinterpretations and explains why we succumb to optical illusions or fall for magic tricks.
Neglect
Neglect is a perceptual disorder in which parts of the body or stimuli are ignored due to a brain lesion. The disorder affects the sides opposite the brain lesion. It usually occurs after lesions in the right parietal lobe. Accordingly, visual, auditory, and somatosensory stimuli on the left side are ignored.
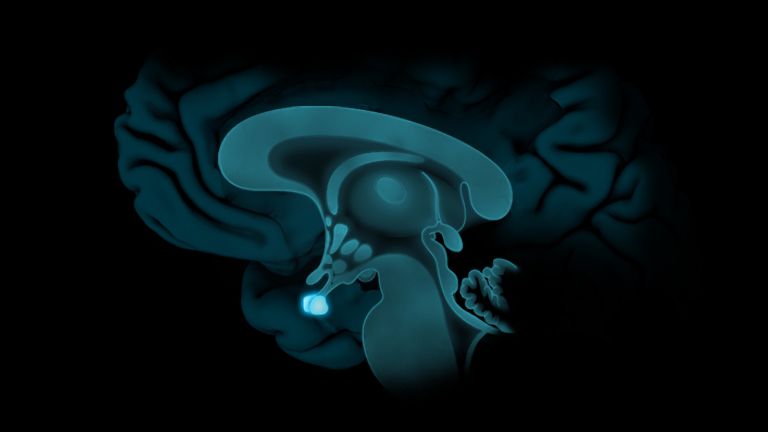
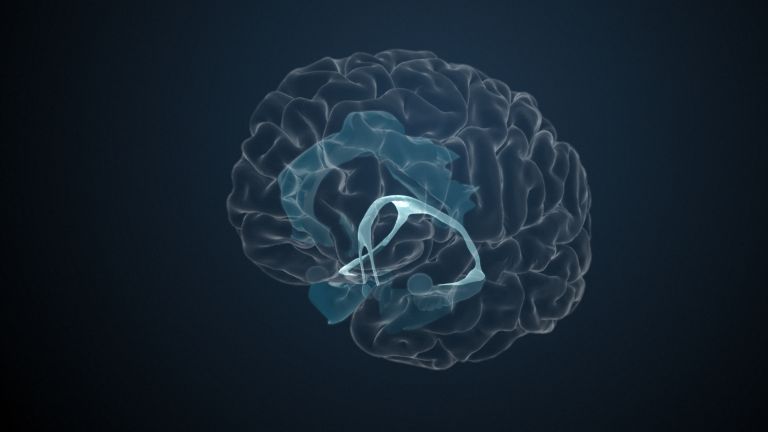
Strange things can happen at the junction between the temporal and parietal lobes, known as the temporoparietal junction (TPJ) – at least when this area is stimulated with electrodes. Olaf Blanke achieved this in Lausanne: he inserted an electrode directly at the end of the Sylvian Fissure in the TPL of a young epilepsy patient. The stimulation caused the patient to feel a “shadow” behind her that mimicked all her actions but also had a will of its own – a kind of ghost. Interestingly, patients with damage in this region often report out-of-body experiences. Some even describe feeling as if they are floating above their own bodies and observing themselves from the outside.
Does this mean that there is a form of spirit or consciousness that can leave the body? Of course, science cannot completely rule this out, but the more likely explanation is that the TPL plays a crucial role in mediating the unity of body and mind by integrating bodily sensations and spatial awareness.
Fissure
The strong folding of the cortex (cerebral cortex) creates fissures – from the Latin: cleft. These clefts can be used to describe individual brain structures. For example, the fissura sylvii separates the temporal lobe from the frontal lobe. Less deep clefts are often referred to as sulci.
The perception of one's own body
Humans are natural dualists: even small children experience themselves – their minds – as separate from their bodies. This intuitive dualism was reinforced by René Descartes (1596−1650) at the beginning of the modern era with the observation that he could cut off his little finger and still be René Descartes. From today's perspective, however, the mind – or rather the brain – and the body form a unity. Nevertheless, the crucial question arises: How can the brain process all the different information from the body and the environment and integrate it into one coherent experience?
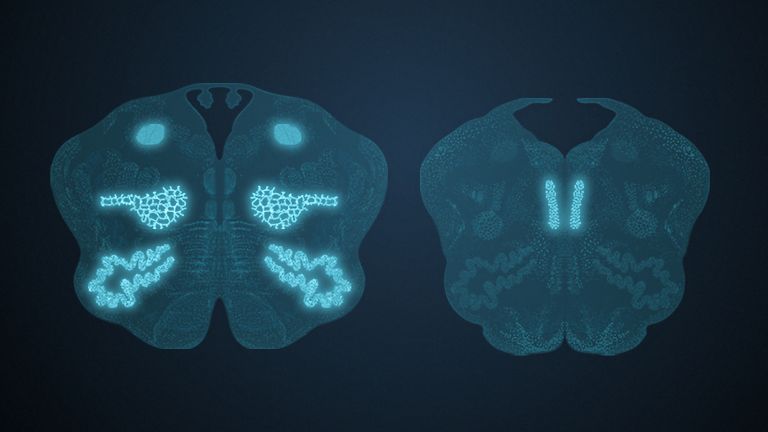
The skin has receptors for temperature and pain, touch and pressure sensations. Most of these signals reach the brain via the so-called protopathic pathway. The epicritic pathway provides finer tactile sensations, as well as information from the musculoskeletal system, i.e., about the activity of tendons and muscles – and thus about the position of individual body parts. This sense is called Proprioception or self-perception. Both pathways run largely through the Spinal cord and Brain stem and cross over to the opposite side at different levels. Thus, the Parietal lobe receives signals from the opposite, contralateral side of the body – the left parietal lobe receives information from the right side of the body and vice versa.
Proprioception
Proprioception is the sense of oneself, or more precisely, the position of one's own limbs and the location of the body in space. It is made possible by certain receptors in muscles, joints, and tendons that constantly send information to the brain. Visual signals and those from the vestibular system are also processed. This enables coordination, balance, and targeted movements without constant visual control.
Spinal cord
medulla spinalis
The spinal cord is the part of the central nervous system located in the spine. It contains both the white matter of the nerve fibers and the gray matter of the cell nuclei. Simple reflexes such as the knee-jerk reflex are already processed here, as sensory and motor neurons are directly connected. The spinal cord is divided into the cervical, thoracic, lumbar, and sacral spinal cord.
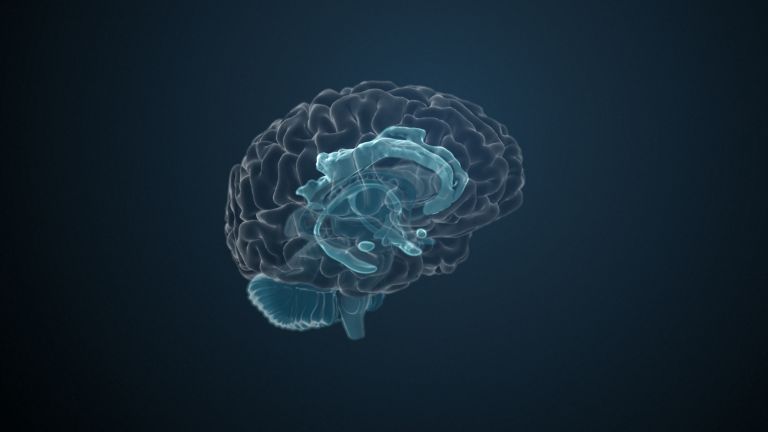
Brain stem
truncus cerebri
The "trunk" of the brain, to which all other brain structures are "attached," so to speak. From bottom to top, it comprises the medulla oblongata, the pons, and the mesencephalon. It transitions into the spinal cord below. It is a center for vital functions such as breathing and heartbeat and contains ascending and descending pathways between the cerebrum, cerebellum, and spinal cord.
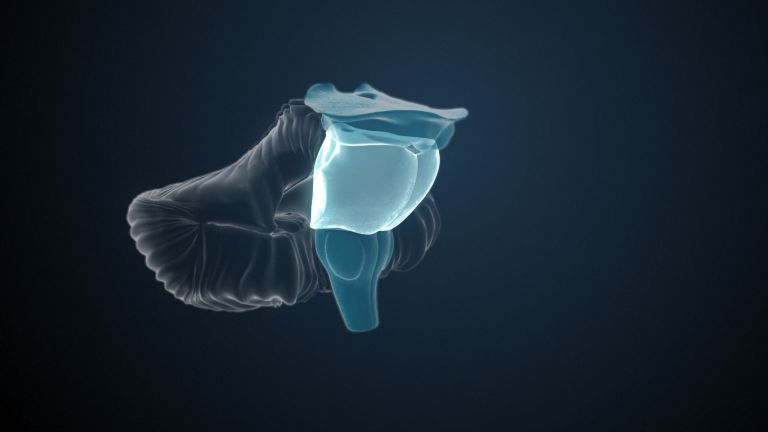
Parietal lobe
Lobus parietalis
The parietal lobe is one of the four large lobes of the cerebral cortex. It is located behind the frontal lobe and above the occipital lobe. Somatosensory processes take place in its anterior region, while sensory information is integrated in its posterior region, enabling the handling of objects and spatial orientation. In addition, the parietal lobe is involved in attention, the recognition of body parts and objects, as well as linguistic and mathematical abilities.
contralateral
Contralateral is a positional term. It means "located on the other side of the body."
The primary somatosensory cortex and its functions
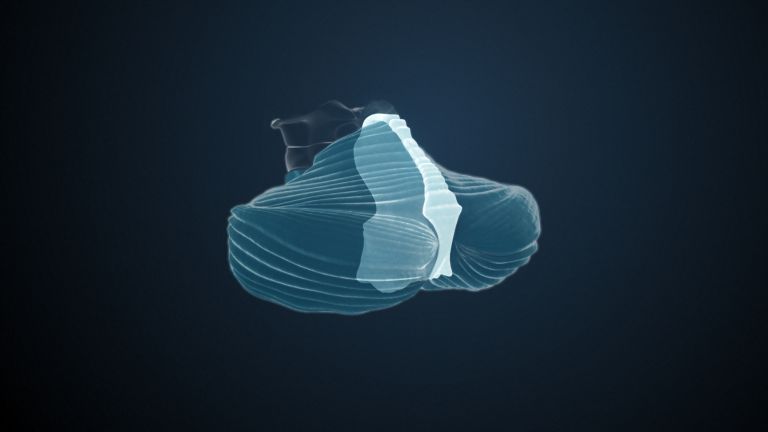
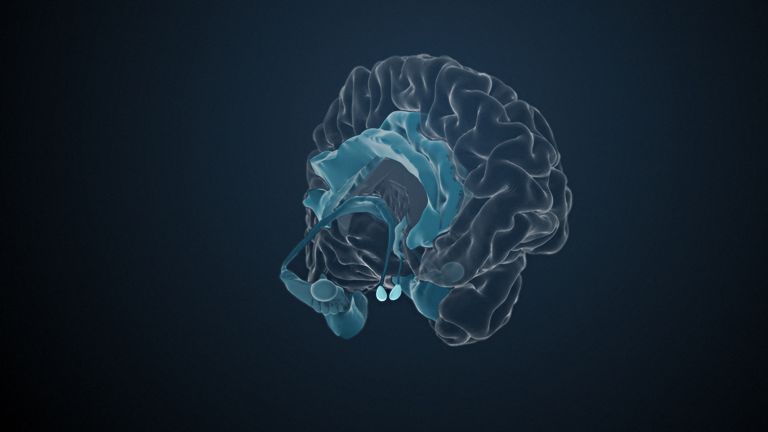
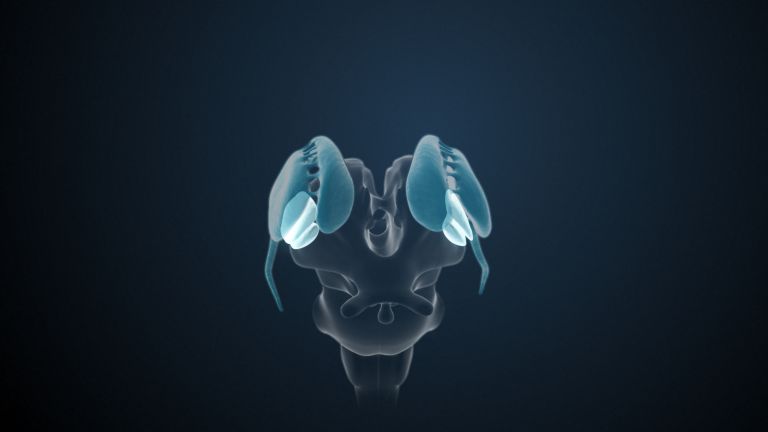
Two larger areas can be distinguished in the Parietal lobe The first is the Primary somatosensory cortex in the Postcentral gyrus – the direct projection site of the protopathic and epicritic pathways. As in the motor cortex, the somatotopic arrangement is preserved, resulting in a neural map of the body. The size of each area reflects the sensitivity of the corresponding structure: hand and head are represented very large, as the Receptor density is particularly high there. The rest of the body is represented rather small.
Depending on their severity, lesions in the postcentral gyrus can lead to impaired sensation in the represented body part. This affects touch, pressure, and temperature. Unfortunately, pain sensation is the least affected.
Parietal lobe
Lobus parietalis
The parietal lobe is one of the four large lobes of the cerebral cortex. It is located behind the frontal lobe and above the occipital lobe. Somatosensory processes take place in its anterior region, while sensory information is integrated in its posterior region, enabling the handling of objects and spatial orientation. In addition, the parietal lobe is involved in attention, the recognition of body parts and objects, as well as linguistic and mathematical abilities.
Primary somatosensory cortex
Area of the cerebrum where haptic stimuli are processed centrally. Anatomically, the somatosensory cortex is located on the first cerebral gyri behind the central sulcus. This is where afferents from sensory cells throughout the body converge. Neurons that evaluate information from neighboring areas of the body are also located next to each other in the somatosensory cortex. Neuroscientists refer to this as somatotopy.S1 is an important station in pain processing – this is where we become aware of the pain stimulus.
Postcentral gyrus
Gyrus postcentralis
The postcentral gyrus is the fold on the surface of the cerebrum located immediately behind the central sulcus. It contains the primary somatosensory cortex, where touch, pressure, temperature, and proprioceptive stimuli are processed.
Receptor
A receptor is a protein, usually located in the cell membrane or inside the cell, that recognizes a specific external signal (e.g., a neurotransmitter, hormone, or other ligand) and causes the cell to trigger a defined response. Depending on the type of receptor, this response can be excitatory, inhibitory, or modulatory.


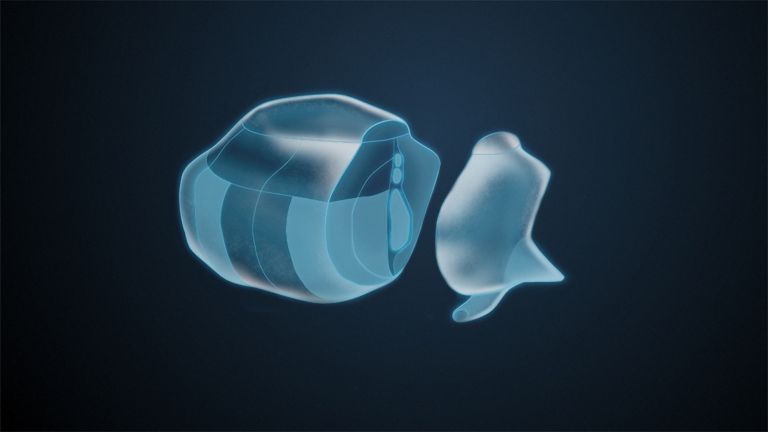









The posterior parietal cortex
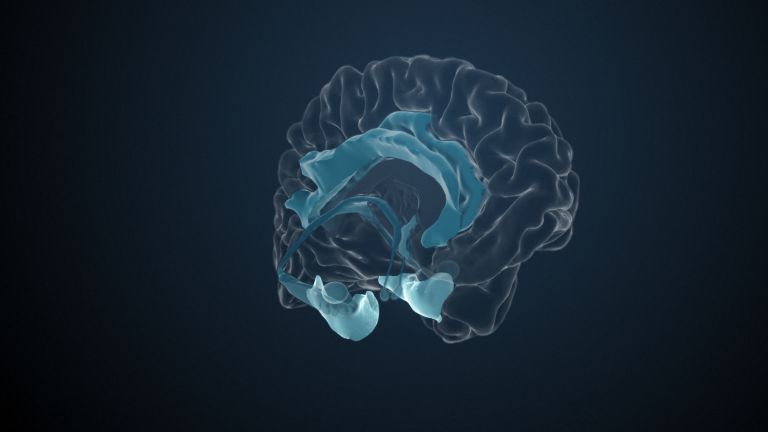
While proprioception, the spatial Perception of one's own body, is the task of the primary somatosensory cortex, the Posterior parietal cortex involves the environment. This is where proprioceptive, auditory, vestibular, and visual information is integrated. The combination of this information creates a three-dimensional image of the environment that is constantly updated. This helps the posterior parietal Cortex to understand where we are in relation to our surroundings and how we can move around in a purposeful and precise manner.
This integration of perception sounds easier than it is: we talk to friends while offering them something to eat: “No thanks, no salad, but I'd like some more sauce...” Here, numerous movements – for example, those of the eyes – must be coordinated with auditory and visual inputs. All of this takes place in a room full of objects: salad bowls and cutlery, plates, and the large pepper mill that is always in the way. The brain is therefore required to create a coherent image of the body and the outside world, and this is decisively shaped by the association cortices of the posterior parietal cortex. One special feature concerns numbers – here, the intraparietal sulcus seems to play an important role.
Clinically, lesions of the posterior Parietal lobe manifest themselves in a variety of ways – and have particular effects due to lateralization effects: if the right side is affected, this can lead to sometimes severe disturbances in orientation. The consequences of right-sided lesions of the lower parietal lobe are particularly striking – they can lead to what is known as left Neglect: Those affected then no longer perceive large parts of the left visual field, for example, they only draw the right side of a clock, only eat what is on the right side of their plate, or even no longer perceive the entire left side of their body. In rare cases, patients even report finding a “foreign leg” in bed. Damage to the dominant hemisphere, which is usually the left hemisphere, can lead to Apraxia: patients are no longer able to perform learned movements such as serving salad. Depending on the location and extent of the lesion, mathematical deficits may also occur, up to and including the loss of abstract thinking.
Perception
The term describes the complex process of gathering and processing information from stimuli in the environment and from the internal states of a living being. The brain combines the information, which is perceived partly consciously and partly unconsciously, into a subjectively meaningful overall impression. If the data it receives from the sensory organs is insufficient for this, it supplements it with empirical values. This can lead to misinterpretations and explains why we succumb to optical illusions or fall for magic tricks.
posterior
A positional term – posterior means "towards the back, located at the rear." In relation to the nervous system, it refers to a direction towards the tail.
Posterior parietal cortex
The posterior parietal lobe receives inputs from numerous visual, auditory, somatosensory, and proprioceptive cortical areas. It integrates this information into an overall spatial picture that enables orientation, spatial attention, and the planning and execution of goal-directed movements.
Cortex
cortex cerebri
Cortex refers to a collection of neurons, typically in the form of a thin surface. However, it usually refers to the cerebral cortex, the outermost layer of the cerebrum. It is 2.5 mm to 5 mm thick and rich in nerve cells. The cerebral cortex is heavily folded, comparable to a handkerchief in a cup. This creates numerous convolutions (gyri), fissures (fissurae), and sulci. Unfolded, the surface area of the cortex is approximately 1,800cm².
Parietal lobe
Lobus parietalis
The parietal lobe is one of the four large lobes of the cerebral cortex. It is located behind the frontal lobe and above the occipital lobe. Somatosensory processes take place in its anterior region, while sensory information is integrated in its posterior region, enabling the handling of objects and spatial orientation. In addition, the parietal lobe is involved in attention, the recognition of body parts and objects, as well as linguistic and mathematical abilities.
Neglect
Neglect is a perceptual disorder in which parts of the body or stimuli are ignored due to a brain lesion. The disorder affects the sides opposite the brain lesion. It usually occurs after lesions in the right parietal lobe. Accordingly, visual, auditory, and somatosensory stimuli on the left side are ignored.
Apraxia
Difficulty performing a purposeful movement, such as grasping a glass or cutting with scissors. Depending on the form of apraxia, speech or facial expressions may also be affected. The cause is not muscle weakness or paralysis, but damage to one or more areas of the brain, e.g., as a result of a stroke. In other cases, however, it is congenital.
First published on September 9, 2011
Last updated on August 15, 2025