Multiple Sclerosis – a Medical Challenge
The wide variety of symptoms makes diagnosing multiple sclerosis difficult. But one thing is clear: the earlier it is detected and the earlier treatment begins, the better the prognosis.
Scientific support: Prof. Dr. Ingo Kleiter, Prof. Dr. Manuel A. Friese, Prof. Dr. Christoph Heesen, Dr. Sina Rosenkranz
Published: 20.02.2026
Difficulty: intermediate
- Based on current knowledge, Multiple sclerosis is likely an autoimmune disease that causes lesions in the central nervous system. Recently, however, there has also been discussion that it could be an inflammatory disease maintained by tissue factors.
- The location of the lesions often determines the patient’s symptoms.
- Neurobiologically, MS is a continuum of inflammation and Neurodegeneration. Clinically, a distinction is made between a relapsing-remitting course and a chronic progressive course. In most cases, a relapsing-remitting course transitions to a chronic progressive course in the later stages. Less commonly, the disease follows a chronic progressive course from the outset without recognizable relapses.
- Thanks to many advances in MS treatment, the majority of patients with MS can now live for long periods without significant limitations. The identification of benign courses through improved diagnostics also plays a role in this.
- Drug treatment is based on three pillars: acute treatment during relapses, immunotherapy, and symptomatic treatment.
- The uncertainty regarding the course of the disease is a major psychological burden for many patients.
- Currently, significant research efforts are underway to identify benign and rapidly progressive courses early on – for example, using biomarkers. This would make it possible to select the appropriate treatment for the patient from the wide range of therapeutic options at an earlier stage.
Multiple sclerosis
encephalomyelitis disseminata
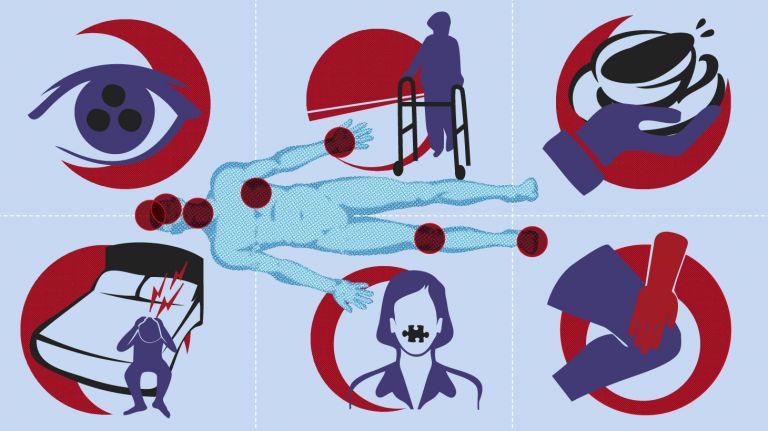
A common neurological disease that predominantly occurs in young adults. For reasons that are still unclear, the body's own cells attack and destroy the myelin sheaths of nerve cells. This can happen throughout the central nervous system, which is why two different multiple sclerosis patients can suffer from very different symptoms. Common symptoms include visual disturbances, numbness in the arms and legs, but also coordination problems, muscle weakness, and bladder problems.
Neurodegeneration
Collective term for diseases in which nerve cells gradually lose their structure or function until they eventually die. In many cases, misfolded proteins are the trigger – such as certain forms of the proteins beta-amyloid and tau in the case of Alzheimer's disease. In other diseases, such as Parkinson's disease or Huntington's disease, proteins within the neurons are not broken down properly. As a result, toxic aggregates are deposited there, leading to the respective disease symptoms. While Huntington's disease is clearly genetic, in Parkinson's and Alzheimer's there appear to be certain gene variants that promote their development. None of these neurodegenerative diseases can be cured at present.
- The numerous medications that have been shown to reduce the relapse rate in MS are divided into three categories based on increasing efficacy:
- The first tier includes interferon-beta preparations – these were the first drugs to demonstrate an effective impact on the long-term clinical course of relapsing-remitting MS. They modulate the immune system and are still used as first-line therapy for mild and moderate forms of the disease. Additionally, there are dimethyl fumarate/diroximel fumarate, glatiramer acetate, and teriflunomide. Current guidelines indicate that these agents reduce relapse rates by approximately 30–50 percent annually compared to a placebo.
- In efficacy class 2, reductions in relapse rates of 50–60 percent on average can be expected. This class includes cladribine and the S1P Receptor modulators fingolimod, ozanimod, and ponesimod.
- Even more effective (Level 3), with a relapse reduction of more than 60 percent compared to placebo, are alemtuzumab, CD20 antibodies (ocrelizumab, ofatumumab, rituximab, ublituximab), and natalizumab.
- However, the choice of medication depends not only on efficacy but also on factors such as tolerability, safety, and potential side effects, which are discussed with patients.
Receptor
A receptor is a protein, usually located in the cell membrane or inside the cell, that recognizes a specific external signal (e.g., a neurotransmitter, hormone, or other ligand) and causes the cell to trigger a defined response. Depending on the type of receptor, this response can be excitatory, inhibitory, or modulatory.
MS is considered the disease with a thousand faces and usually manifests between the ages of 20 and 40. It can sometimes take some time before a diagnosis is reached. The wide variety of symptoms associated with the disease complicates diagnosis. In neurological evaluation, specific techniques are used to confirm the diagnosis and rule out other conditions.
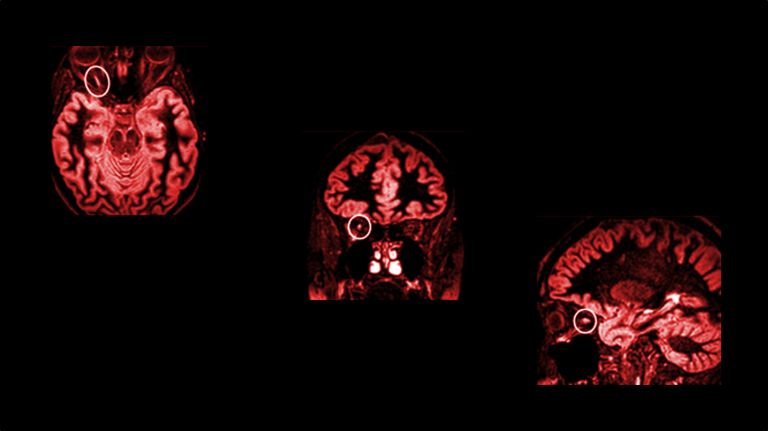
Magnetic resonance imaging (MRI) reveals areas of inflammation in MS, and an analysis of the Cerebrospinal fluid (CSF) shows signs of inflammation. When an initial episode suggesting MS occurs, it is referred to as a clinically isolated syndrome (CIS). This can include, for example, visual disturbances, gait disturbances, or numbness. In about 30 percent of patients, MS begins with a visual disturbance in the form of blurred or foggy vision, which may be caused by inflammation of one of the two optic nerves. In about two-thirds of patients, clinically isolated syndrome is a precursor to MS.Research has previously assumed that MS is an autoimmune disease. According to this theory, misdirected immune cells are supposed to attack, among other things, the cells that form the insulating sheath of the nerves in the brain or Spinal cord – the so-called Myelin sheaths. Deprived of their insulation, the nerves transmit information more slowly or not at all. Furthermore, this can lead to irreversible damage to the nerve cell tracts (axons) and the loss of neurons. However, this model has recently been called into question, and some researchers doubt that the loss of the myelin sheath is actually the cause or rather merely an irrelevant consequence of inflammation.
Multiple sclerosis
encephalomyelitis disseminata
A common neurological disease that predominantly occurs in young adults. For reasons that are still unclear, the body's own cells attack and destroy the myelin sheaths of nerve cells. This can happen throughout the central nervous system, which is why two different multiple sclerosis patients can suffer from very different symptoms. Common symptoms include visual disturbances, numbness in the arms and legs, but also coordination problems, muscle weakness, and bladder problems.
Magnetic resonance imaging
Magnetic resonance imaging scanner
A device used by medical professionals for magnetic resonance imaging (MRI). MRI is an imaging technique used to diagnose malformations in various tissues or organs of the body. This method is particularly effective for imaging parts of the body that contain a lot of water. Patients are placed in a tube (scanner) and exposed to a strong magnetic field. However, they are not exposed to X-rays or other forms of ionizing radiation.
Cerebrospinal fluid
liquor cerebrospinalis
A clear fluid that fills the ventricular system and bathes the brain and spinal cord in the subarachnoid space, protecting them from impact. Three to five times a day, 100 to 160 ml of fluid is renewed by the choroid plexus. Certain diseases are reflected in the composition of the cerebrospinal fluid.
Spinal cord
medulla spinalis
The spinal cord is the part of the central nervous system located in the spine. It contains both the white matter of the nerve fibers and the gray matter of the cell nuclei. Simple reflexes such as the knee-jerk reflex are already processed here, as sensory and motor neurons are directly connected. The spinal cord is divided into the cervical, thoracic, lumbar, and sacral spinal cord.
Myelin
Myelin is a fatty substance produced by glial cells. It envelops the axons (long, fiber-like extensions) of nerve cells and insulates them, preventing messages from passing uncontrollably to neighboring nerve cells. This also greatly accelerates conduction velocity.
The disease with 1,000 faces
There are several theories as to why the immune system destroys the nerve sheaths, but researchers have not yet reached a consensus. There may also be several different causes.
New study results have led to the realization that early initiation of immunotherapy can reduce the progression of disability. This also means starting therapy as early as the CIS stage, because this can prevent further events. Symptoms are not yet very noticeable at this stage, as the brain can still compensate for the damage. That is why CIS patients generally do very well for many years at first. However, as the disease progresses, autoimmune-mediated inflammatory reactions can occur anywhere in the brain or spinal cord, which can ultimately lead to a variety of symptoms:
- If parts of the Cerebellum become inflamed, gait disturbances, coordination problems, and dizziness are the most common symptoms.
- If the brainstem is affected, symptoms may include swallowing difficulties, speech disorders (slurred speech), balance problems, sensory disturbances, and paralysis. Paralysis is often associated with a feeling of stiffness caused by spasticity: a constant tension in the muscles that can lead to cramping.
- Inflammation in the Spinal cord can also lead to sensory disturbances and paralysis, as well as bladder and bowel dysfunction and sexual dysfunction. Bladder dysfunction usually manifests as an urge to urinate that is difficult to control or as problems emptying the bladder.
- Finally, pain pathways in the central nervous system may also be affected. Since inflammation often heals with scarring, the pain may persist permanently.
Not only the symptoms but also the course of the disease can vary from patient to patient. In over 85 percent of patients, MS initially follows a relapsing-remitting course. This means that neurological impairments appear in the form of sudden worsening episodes (= relapses) and alternate with symptom-free or low-symptom phases. Initially, the relapses usually resolve completely; in the later stages, only partially.
Without treatment, at least half of patients used to experience a steady increase in disability over the long term (secondary progressive course). Thanks to new treatments, the proportion of patients who develop severe disabilities over time and are no longer able to walk has dropped significantly. Only about 10 to 15 percent require a permanent mobility device or wheelchair after approximately 20 years.
In a smaller proportion of patients – about 10 to 15 percent – the disease progresses without relapses from the outset; instead, symptoms increase steadily and insidiously (primary progressive course). Many of these patients suffer from a spastic gait disorder that worsens over the years. This form of the disease is more common in patients in whom the disease begins after the age of 40.
MS is incurable, but a wide range of treatments is now available. During an acute relapse, symptoms are treated with high-dose corticosteroids; if this is unsuccessful, plasma exchange (plasmapheresis or immunoadsorption) is used. Immunomodulators are employed to influence the long-term course of the disease. It has been shown that starting therapy as early as possible yields the greatest benefit – presumably because many permanent damages caused by relapses can be prevented.
Most patients therefore receive dimethyl fumarate after diagnosis, which is taken as a tablet twice daily, glatiramer acetate (injected under the skin), teriflunomide (tablet), or one of several genetically engineered preparations containing the active ingredient interferon beta-1a or interferon beta-1b, with which the longest experience has been gained. They all have a modulating effect on the immune system and reduce the relapse rate by up to 50 percent.
If the effect of these substances is insufficient, additional substances may be considered: The most common are the genetically engineered antibodies ocrelizumab, ofatumumab, rituximab, and ublituximab, which specifically bind to the CD20 antigen on the surface of B-lymphocytes. This eliminates these cells from the blood. Since B cells play a key role in activating the inflammatory cascade, the attack on the nervous system is highly effectively halted.
The S1P Receptor modulators fingolimod, ozanimod, siponimod, and ponesimod have a different target: They “trap” immune cells in the lymph nodes, thereby preventing them from entering the central nervous system and triggering inflammation there.
Cladribine is a medication that is not administered continuously but in short cycles to effectively “reset” the immune system. It interferes with the DNA metabolism of lymphocytes, leading to their degradation. The antibody alemtuzumab works on the same principle of “selective immune reconstitution therapy.” However, its extremely high efficacy comes at the cost of severe side effects, so alemtuzumab is generally only used when other escalation therapies have failed.
The antibody natalizumab is in a class of its own; it is administered as an infusion every four to six weeks. By binding to the immune cell surface molecule VLA-4, natalizumab prevents these cells from leaving the blood vessels and entering the brain tissue. Its biggest drawback is that – much more frequently than with other drugs – it can activate the JC virus as a side effect, which in very rare cases leads to a life-threatening brain infection.
In addition to regulating the immune system, symptom management is also part of treatment, for example for Depression. “MS research has made progress in all areas in recent years: both in immunotherapy and symptom management. For example, the treatment of spasticity has improved dramatically – cannabinoids are being studied for this purpose and are showing effectiveness,” says Dr. Dieter Pöhlau, Vice Chairman of the German Multiple sclerosis Society (DMSG).
Cerebellum
Cerebellum
The cerebellum is an important part of the brain, located at the back of the brain stem and below the occipital lobe. It consists of two cerebellar hemispheres covered by the cerebellar cortex and plays an important role in motor processes, among other things. It develops from the rhombencephalon.
Spinal cord
medulla spinalis
The spinal cord is the part of the central nervous system located in the spine. It contains both the white matter of the nerve fibers and the gray matter of the cell nuclei. Simple reflexes such as the knee-jerk reflex are already processed here, as sensory and motor neurons are directly connected. The spinal cord is divided into the cervical, thoracic, lumbar, and sacral spinal cord.
Receptor
A receptor is a protein, usually located in the cell membrane or inside the cell, that recognizes a specific external signal (e.g., a neurotransmitter, hormone, or other ligand) and causes the cell to trigger a defined response. Depending on the type of receptor, this response can be excitatory, inhibitory, or modulatory.
Depression
A mental illness whose main symptoms are sadness and a loss of joy, motivation, and interest. Current classification systems distinguish between different types of depression.
Multiple sclerosis
encephalomyelitis disseminata
A common neurological disease that predominantly occurs in young adults. For reasons that are still unclear, the body's own cells attack and destroy the myelin sheaths of nerve cells. This can happen throughout the central nervous system, which is why two different multiple sclerosis patients can suffer from very different symptoms. Common symptoms include visual disturbances, numbness in the arms and legs, but also coordination problems, muscle weakness, and bladder problems.





Significant Psychological Stress: The Uncertainty
For an MS patient, coping with uncertainty is a major challenge. No one can tell them exactly how their disease will progress. After the first symptoms appear, it can take years before the next relapse. “The psychological effects of MS should not be underestimated. No matter how well the patient is managed, if they just sit at home anxiously, fearing the next relapse, their quality of life is still poor.” Specialized mental health support programs are designed to prevent this by teaching patients how to cope with the stress. The DMSG was the first association in Germany to develop such a program, but it has since become a central component of therapy in many neurological clinics.
Many questions remain unanswered. For instance, intensive work is underway to predict the course of MS, according to Reinhard Hohlfeld, Professor Emeritus at the Institute for Clinical Neuroimmunology at Ludwig Maximilian University of Munich: “There are also still no hard criteria today that can be used to predict response to therapy. For example, one would hope for immunological markers or MRI criteria that could be used to determine an individual’s prognosis.”
More than 80,000 scientific papers on MS have been published over the past 30 years – half of them in the last decade alone. And yet (or because of?) this wealth of data, there are still gaps in the map of MS research. One of the most important questions currently is how the disease progresses and whether this process can be halted with medication.
Scientists, doctors, and above all, patients will need a great deal of patience until the final mysteries of this disease are solved, but at the same time, they can be certain that they are living in the most hopeful era in the history of MS.
Further reading
- German Society of Neurology (DGN), German Multiple sclerosis Society (DMSG) (Eds.). S2k Guideline “Diagnosis and Treatment of Multiple Sclerosis, Neuromyelitis Optica Spectrum, and MOG-IgG-Associated Diseases.” Version 8.0 (Living Guideline), URL: https://www.dgn.org/leitlinie/diagnose-und-therapie-der-multiplen-sklerose-neuromyelitis-optica-spektrum-erkrankungen-und-mog-igg-assoziierten-erkrankungen (accessed on April 6, 2026).
- Jakimovski D, Bittner S, Zivadinov R, et al. Multiple sclerosis. Lancet. 2024;403(10422):183-202. doi:10.1016/S0140-6736(23)01473-3
Multiple sclerosis
encephalomyelitis disseminata
A common neurological disease that predominantly occurs in young adults. For reasons that are still unclear, the body's own cells attack and destroy the myelin sheaths of nerve cells. This can happen throughout the central nervous system, which is why two different multiple sclerosis patients can suffer from very different symptoms. Common symptoms include visual disturbances, numbness in the arms and legs, but also coordination problems, muscle weakness, and bladder problems.
Originally published on May 30, 2017
Last updated on February 20, 2026
