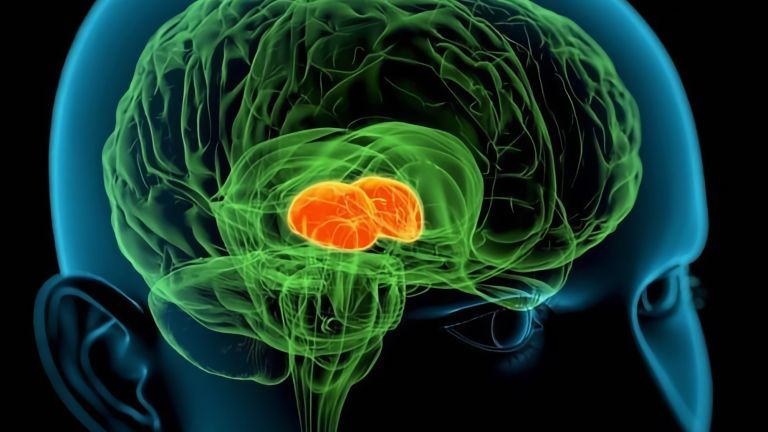
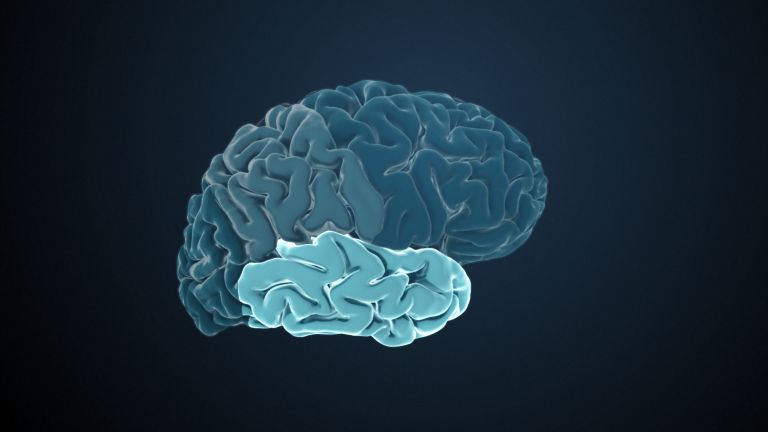
The Parietal Lobe

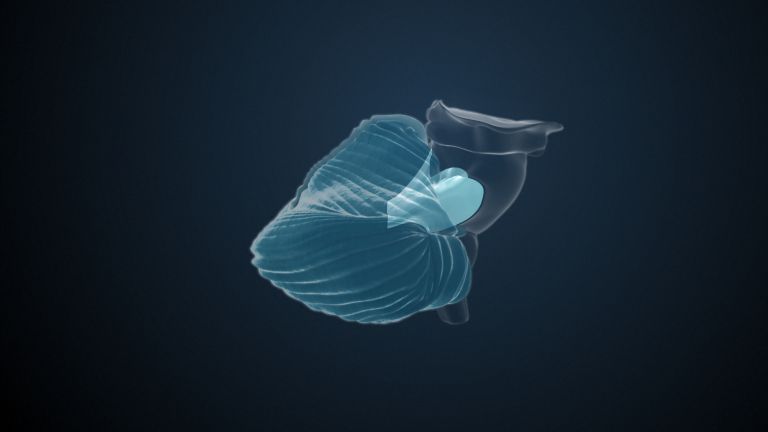
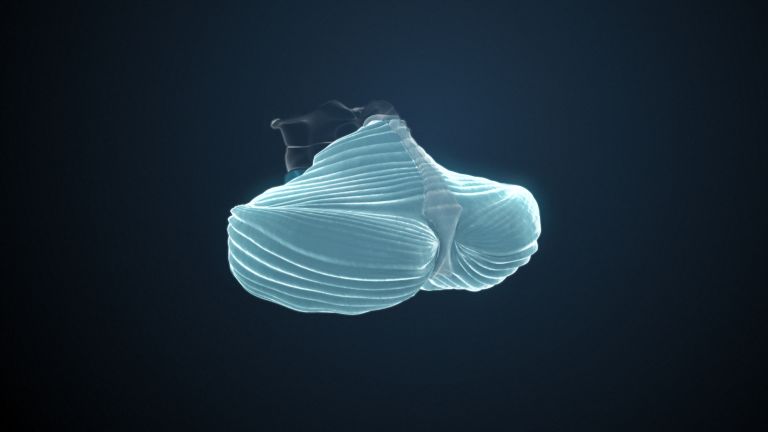
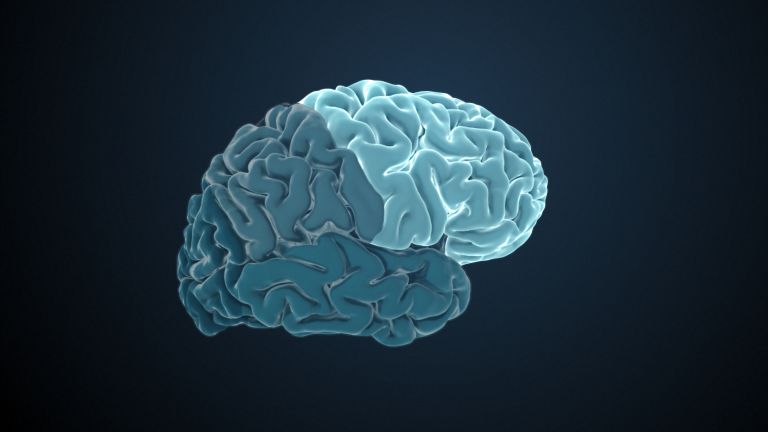
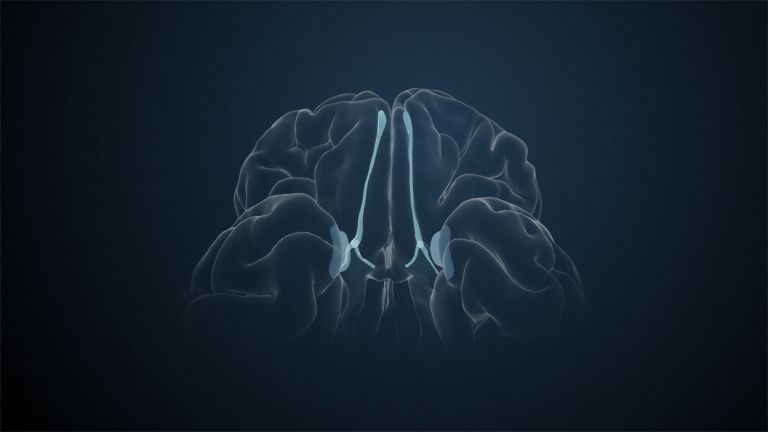
The parietal lobe is located behind the frontal lobe and is separated from it by the central sulcus. Two important nerve pathways that transmit bodily sensations such as pain, temperature, and touch end in the parietal lobe. However, the functions of the parietal lobe extend far beyond the body.
Wissenschaftliche Betreuung: Prof. Dr. Herbert Schwegler, Prof. Dr. Anne Albrecht
Veröffentlicht: 18.09.2025
Niveau: mittel
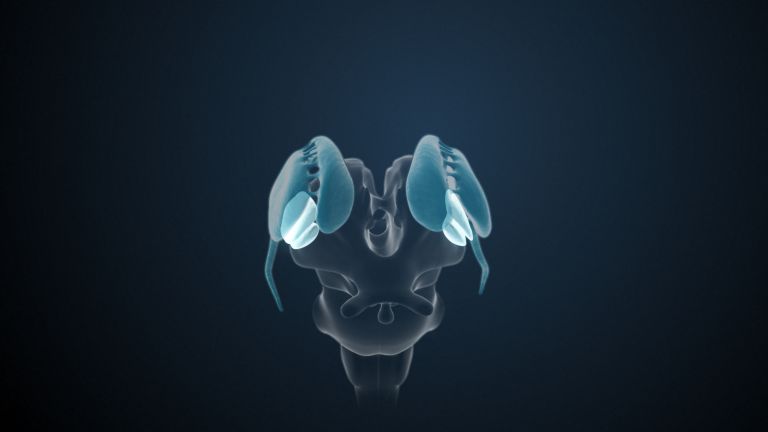
Die Hauptfunktion des Parietallappens ist die Verarbeitung von Informationen unserer somatosensorischen Wahrnehmung: Was fühlt der Körper (z. B. Berührung, Schmerz, Temperatur) und wo und in welcher Position befinden sich die eigenen Gliedmaßen? Während dies im somatosensorischen Cortex geschieht, setzt der hintere Bereich des Parietallappens diese Informationen in Beziehung zur nahen und fernen Umgebung. Schäden in diesen Bereichen können zu einem sogenannten Neglect führen – zu Schwierigkeiten beim Erkennen der eigenen Gliedmaßen oder einer Hälfte der Umwelt.
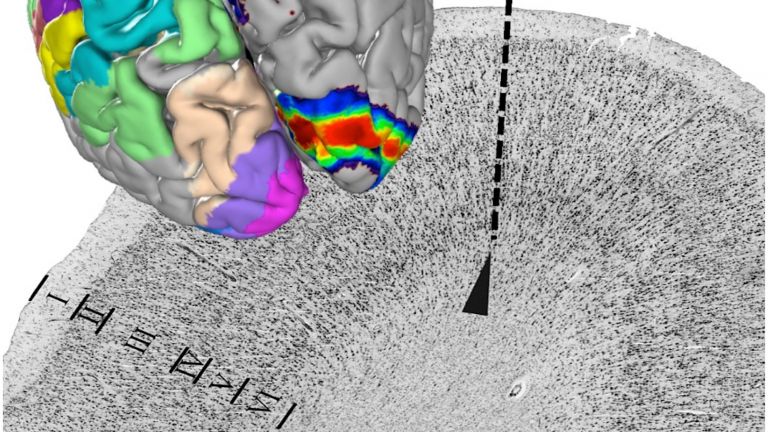
Cortex
Großhirnrinde/Cortex cerebri/cerebral cortex
Cortex bezeichnet eine Ansammlung von Neuronen, typischerweise in Form einer dünnen Oberfläche. Meist ist allerdings der Cortex cerebri gemeint, die äußerste Schicht des Großhirns. Sie ist 2,5 mm bis 5 mm dick und reich an Nervenzellen. Die Großhirnrinde ist stark gefaltet, vergleichbar einem Taschentuch in einem Becher. So entstehen zahlreiche Windungen (Gyri), Spalten (Fissurae) und Furchen (Sulci). Ausgefaltet beträgt die Oberfläche des Cortex ca 1.800 cm2.
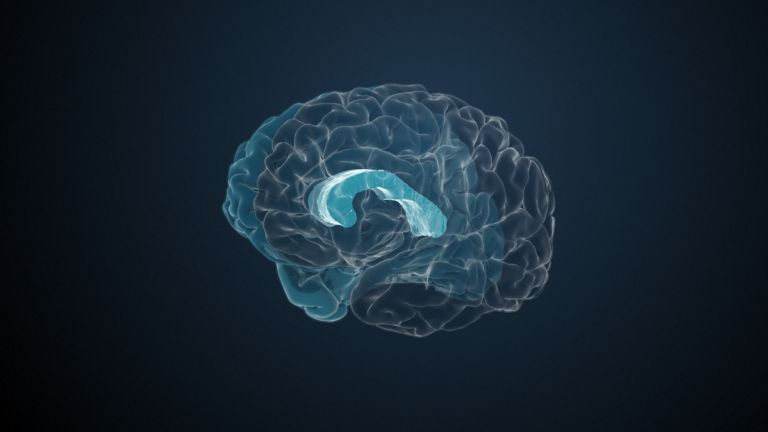
Am Übergang von Temporal- und Parietallappen, der so genannten temporoparietale Übergang (TPJ), können merkwürdige Dinge geschehen – zumindest, wenn man diesen Bereich mit Elektroden stimuliert. Dies gelang Olaf Blanke in Lausanne: Er führte eine Elektrode direkt am Ende der Sylvischen Fissur in den TPL einer jungen Epilepsiepatientin ein. Durch die Stimulation spürte die Patientin einen „Schatten“ hinter sich, der all ihre Handlungen nachahme, der aber auch einen eigenen Willen hätte – eine Art Geist. Interessanterweise berichten Patienten mit Schäden in dieser Region häufig von außerkörperlichen Erfahrungen. Manche beschreiben sogar, dass sie das Gefühl haben, über ihrem eigenen Körper zu schweben und sich selbst von außen zu beobachten.
Bedeutet dies, dass es eine Form von Geistern oder ein Bewusstsein gibt, das den Körper verlassen kann? Gänzlich ausschließen kann die Naturwissenschaft dies natürlich nicht, doch die wahrscheinlichere Erklärung ist, dass die TPL eine entscheidende Rolle bei der Vermittlung der Einheit von Körper und Geist spielt, indem sie Körperempfindungen und räumliches Bewusstsein integriert.
The perception of one's own body
Humans are natural dualists: even small children experience themselves – their minds – as separate from their bodies. This intuitive dualism was reinforced by René Descartes (1596−1650) at the beginning of the modern era with the observation that he could cut off his little finger and still be René Descartes. From today's perspective, however, the mind – or rather the brain – and the body form a unity. Nevertheless, the crucial question arises: How can the brain process all the different information from the body and the environment and integrate it into one coherent experience?
The skin has receptors for temperature and pain, touch and pressure sensations. Most of these signals reach the brain via the so-called protopathic pathway. The epicritic pathway provides finer tactile sensations, as well as information from the musculoskeletal system, i.e., about the activity of tendons and muscles – and thus about the position of individual body parts. This sense is called proprioception or self-perception. Both pathways run largely through the spinal cord and brain stem and cross over to the opposite side at different levels. Thus, the parietal lobe receives signals from the opposite, contralateral side of the body – the left parietal lobe receives information from the right side of the body and vice versa.
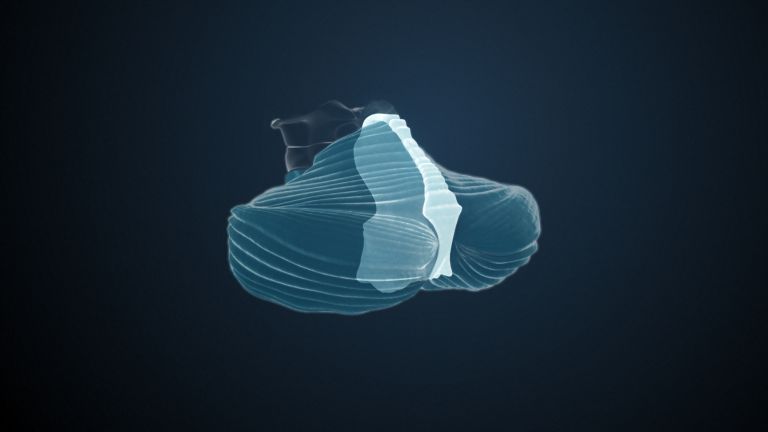
The primary somatosensory cortex and its functions
Two larger areas can be distinguished in the parietal lobe. The first is the primary somatosensory cortex in the postcentral gyrus – the direct projection site of the protopathic and epicritic pathways. As in the motor cortex, the somatotopic arrangement is preserved, resulting in a neural map of the body. The size of each area reflects the sensitivity of the corresponding structure: hand and head are represented very large, as the receptor density is particularly high there. The rest of the body is represented rather small.
Depending on their severity, lesions in the postcentral gyrus can lead to impaired sensation in the represented body part. This affects touch, pressure, and temperature. Unfortunately, pain sensation is the least affected.











The posterior parietal cortex
While proprioception, the spatial perception of one's own body, is the task of the primary somatosensory cortex, the posterior parietal cortex involves the environment. This is where proprioceptive, auditory, vestibular, and visual information is integrated. The combination of this information creates a three-dimensional image of the environment that is constantly updated. This helps the posterior parietal cortex to understand where we are in relation to our surroundings and how we can move around in a purposeful and precise manner.
This integration of perception sounds easier than it is: we talk to friends while offering them something to eat: “No thanks, no salad, but I'd like some more sauce...” Here, numerous movements – for example, those of the eyes – must be coordinated with auditory and visual inputs. All of this takes place in a room full of objects: salad bowls and cutlery, plates, and the large pepper mill that is always in the way. The brain is therefore required to create a coherent image of the body and the outside world, and this is decisively shaped by the association cortices of the posterior parietal cortex. One special feature concerns numbers – here, the intraparietal sulcus seems to play an important role.
Clinically, lesions of the posterior parietal lobe manifest themselves in a variety of ways – and have particular effects due to lateralization effects: if the right side is affected, this can lead to sometimes severe disturbances in orientation. The consequences of right-sided lesions of the lower parietal lobe are particularly striking – they can lead to what is known as left neglect: Those affected then no longer perceive large parts of the left visual field, for example, they only draw the right side of a clock, only eat what is on the right side of their plate, or even no longer perceive the entire left side of their body. In rare cases, patients even report finding a “foreign leg” in bed. Damage to the dominant hemisphere, which is usually the left hemisphere, can lead to apraxia: patients are no longer able to perform learned movements such as serving salad. Depending on the location and extent of the lesion, mathematical deficits may also occur, up to and including the loss of abstract thinking.
First published on September 9, 2011
Last updated on August 15, 2025