When Consciousness fails

Conscious perception of our surroundings requires several subcortical and cortical brain structures that process and classify sensory impressions. If one of these structures fails, part of our consciousness disappears with it.
Scientific support: Prof. Dr. Niels Birbaumer
Published: 13.06.2025
Difficulty: intermediate
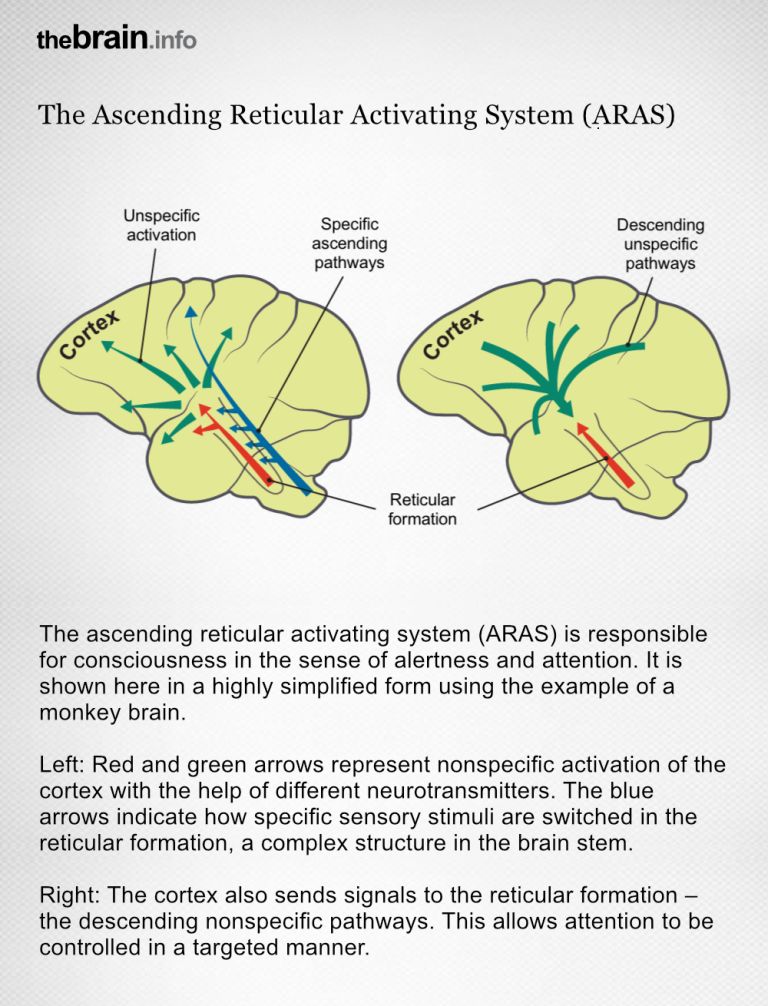
- The ascending reticular activating system (ARAS) maintains numerous nerve connections to the cerebral Cortex. These nerve fibers influence the degree of activation, i.e., the alertness of the brain.
- The thalamus, and in particular the Nucleus reticularis thalami, is “the gateway to consciousness”. All sensory impressions except the sense of smell are interconnected in this core area and can be amplified or attenuated by regions of the Cerebrum. We call this selective attention.
- In the so-called vegetative or non-reactive state, the person is awake, their reticular activation is functioning, but they have no conscious Perception: the connection between the parietal cortex and the Prefrontal cortex is destroyed.
- Injuries in the area of the cerebral cortex result in partial loss of sensory impressions. If an entire Hemisphere is affected, the person affected only perceives half of their surroundings.
- It is still unclear exactly when the different sensory impressions reach consciousness. The duration of transmission probably depends on the complexity of the sensory impression. In the case of simple stimuli, studies of evoked brain potentials usually assume a duration of approximately 220 milliseconds until the stimuli become conscious.
Cortex
cortex cerebri
Cortex refers to a collection of neurons, typically in the form of a thin surface. However, it usually refers to the cerebral cortex, the outermost layer of the cerebrum. It is 2.5 mm to 5 mm thick and rich in nerve cells. The cerebral cortex is heavily folded, comparable to a handkerchief in a cup. This creates numerous convolutions (gyri), fissures (fissurae), and sulci. Unfolded, the surface area of the cortex is approximately 1,800cm².
Nucleus
In cell biology, the nucleus in a cell is the cell nucleus, which contains the chromosomes, among other things. In neuroanatomy, the nucleus in the nervous system refers to a collection of cell bodies – known as gray matter in the central nervous system and ganglia in the peripheral nervous system.
Cerebrum
telencephalon
The cerebrum comprises the cerebral cortex (gray matter), the nerve fibers (white matter), and the basal ganglia. It is the largest part of the brain. The cortex can be divided into four cortical areas: the temporal lobe, frontal lobe, occipital lobe, and parietal lobe.
Its functions include the coordination of perception, motivation, learning, and thinking.
Perception
The term describes the complex process of gathering and processing information from stimuli in the environment and from the internal states of a living being. The brain combines the information, which is perceived partly consciously and partly unconsciously, into a subjectively meaningful overall impression. If the data it receives from the sensory organs is insufficient for this, it supplements it with empirical values. This can lead to misinterpretations and explains why we succumb to optical illusions or fall for magic tricks.
Prefrontal cortex
Prefrontal cortex
The prefrontal cortex (PFC) forms the front part of the frontal lobe and is one of the brain's most important integration and control centers. It receives highly processed information from many other areas of the cortex and is responsible for planning, controlling, and flexibly adapting one's own behavior. Its central tasks include executive functions, working memory, emotion regulation, and decision-making. In addition, the PFC plays an important role in the cognitive evaluation and modulation of pain.
Hemisphere
The cerebrum and cerebellum each consist of two halves – the right and left hemispheres. In the cerebrum, they are connected by three pathways (commissures). The largest commissure is the corpus callosum.
All sensory impressions must first pass through the thalamus before they can become conscious. But there is one exception: the sense of smell. Its signals take a shortcut directly to the Limbic system There, every nuance of smell arrives unfiltered – whether pleasant or unpleasant. The limbic system then links these with the feelings that prevail during smelling. Smells are therefore a particularly good way of bringing back memories. If the specific scent or smell is perceived again later, the corresponding Memory from childhood and youth often resurfaces.
Limbic system
The limbic system is a functional unit in the brain. It consists of interconnected structures, primarily in the cerebrum and diencephalon. The structures assigned to the system vary depending on the source, but the most important components are the hippocampus, amygdala, cingulate gyrus, septum, and mammillary bodies. The limbic system is involved in autonomic and visceral processes as well as in mechanisms of emotion, memory, and learning. Some authors mistakenly reduce the limbic system to the emotional world by referring to it as the "emotional brain."
Memory
Memory is a generic term for all types of information storage in the organism. In addition to pure retention, this also includes the absorption of information, its organization, and retrieval.
The brain is constantly under fire. Countless sensory impressions bombard our nerve cells every day and must then be evaluated and sorted. Fortunately, not every sensory stimulus makes it into our active consciousness. Just imagine how annoying it would be if every single sensory Perception immediately popped into our minds: “I'm warm. It smells like coffee. My colleague is typing on his keyboard. It still smells like coffee...” Instead, we usually only consciously perceive what seems new or important. For example, when our esteemed colleague spills coffee on his keyboard.
However, to access the important information, all the unimportant information must first be briefly evaluated. For our brain to process all the many sensory stimuli, it requires a complex neural system that hierarchically controls our selective Attention. The signal “coffee on the keyboard,” for example, requires the thalamus and Neocortex to work together. The subcortical motor regions of the Basal ganglia – especially the anterior Striatum – are also involved in conscious attention, helping to select the appropriate responses.
Perception
The term describes the complex process of gathering and processing information from stimuli in the environment and from the internal states of a living being. The brain combines the information, which is perceived partly consciously and partly unconsciously, into a subjectively meaningful overall impression. If the data it receives from the sensory organs is insufficient for this, it supplements it with empirical values. This can lead to misinterpretations and explains why we succumb to optical illusions or fall for magic tricks.
Attention
Attention
Attention serves as a tool for consciously perceiving internal and external stimuli. We achieve this by focusing our mental resources on a limited number of stimuli or pieces of information. While some stimuli automatically attract our attention, we can select others in a controlled manner. The brain also unconsciously processes stimuli that are not currently the focus of our attention.
Neocortex
The neocortex is the phylogenetically youngest part of the cerebral cortex. Since it is structured relatively uniformly in six layers, it is also referred to as the isocortex.
Basal ganglia
Nuclei basales
The basal ganglia are a group of subcortical nuclei (located beneath the cerebral cortex) in the telencephalon. The basal ganglia include the globus pallidus and the striatum, and, depending on the author, other structures such as the substantia nigra and the subthalamic nucleus. The basal ganglia are primarily associated with voluntary motor function, but they also influence motivation, learning, and emotion.
Striatum
Corpus striatum
The striatum is a central structure of the basal ganglia. It consists of the caudate nucleus and putamen; the nucleus accumbens is also functionally part of it as its ventral portion. As the most important input structure of the basal ganglia, the striatum plays an essential role in controlling movement sequences as well as in cognition, motivational processes, and the reward system.
Cortex
cortex cerebri
Cortex refers to a collection of neurons, typically in the form of a thin surface. However, it usually refers to the cerebral cortex, the outermost layer of the cerebrum. It is 2.5 mm to 5 mm thick and rich in nerve cells. The cerebral cortex is heavily folded, comparable to a handkerchief in a cup. This creates numerous convolutions (gyri), fissures (fissurae), and sulci. Unfolded, the surface area of the cortex is approximately 1,800cm².
Well-connected activation system
The basis of this system is the ascending reticular activating system, or ARAS for short. This is a network with a large number of nerve nuclei. The ARAS extends from the Midbrain via the “thalamus” interface to the Cerebrum. The cerebrum itself, with its parietal and prefrontal cortex, is involved in the selection and conscious Perception of stimuli and, together with the basal ganglia, determines which response is selected. Therefore, even without feedback on the success of the movements, conscious thinking slowly fails.
This extensive networking is essential because the ARAS influences the activation status of all brain systems. “Its impulses prepare the brain for the reception and processing of new information,” explains Wolf Singer. Attention and the arousal function are primarily mediated by three transmitter systems: norepinephrine, acetylcholine, and Serotonin. Norepinephrine and Acetylcholine activate the thalamus and thus the receptivity of the cerebral Cortex. Serotonin slows down the flow of information. This makes the ARAS indispensable for all types of perception. If it is destroyed, the affected person falls into a coma.
Coma is the most severe form of consciousness disorder. It often occurs in cases of traumatic injury to various parts of the ARAS, but can also occur in cases of extensive lesions of the cerebral cortex, especially after interruption of the connection between the parietal cortex and the Prefrontal cortex In a coma, even strong external stimuli can no longer wake the affected person. No bright light, no loud ringing, not even pain penetrates the cerebral cortex. This is also evident in the electroencephalogram (EEG), which is usually severely and permanently slowed down.
Midbrain
mecencephalon
The midbrain is the uppermost section of the brain stem. Its regions are located around the aqueduct, a canal filled with cerebrospinal fluid. Prominent structures include the tectum, tegmentum, and substantia nigra.
Cerebrum
telencephalon
The cerebrum comprises the cerebral cortex (gray matter), the nerve fibers (white matter), and the basal ganglia. It is the largest part of the brain. The cortex can be divided into four cortical areas: the temporal lobe, frontal lobe, occipital lobe, and parietal lobe.
Its functions include the coordination of perception, motivation, learning, and thinking.
Perception
The term describes the complex process of gathering and processing information from stimuli in the environment and from the internal states of a living being. The brain combines the information, which is perceived partly consciously and partly unconsciously, into a subjectively meaningful overall impression. If the data it receives from the sensory organs is insufficient for this, it supplements it with empirical values. This can lead to misinterpretations and explains why we succumb to optical illusions or fall for magic tricks.
Attention
Attention
Attention serves as a tool for consciously perceiving internal and external stimuli. We achieve this by focusing our mental resources on a limited number of stimuli or pieces of information. While some stimuli automatically attract our attention, we can select others in a controlled manner. The brain also unconsciously processes stimuli that are not currently the focus of our attention.
Serotonin
A neurotransmitter that acts as a messenger in the transmission of information between neurons at their synapses. It is primarily produced in the raphe nuclei of the brain stem and plays a key role in sleep and alertness, as well as emotional well-being.
Acetylcholine
Acetylcholine is one of the most important neurotransmitters in the nervous system. In the central nervous system, it is involved in attention, learning, and memory; in the peripheral nervous system, it transmits excitation from nerves to muscles at the neuromuscular end plates and controls processes of the autonomic nervous system, i.e., the sympathetic and parasympathetic parts. Areas in which acetylcholine acts as a messenger substance are called cholinergic. It was the first neurotransmitter to be discovered, identified in 1921 by Otto Loewi in the heart of a frog.
Cortex
cortex cerebri
Cortex refers to a collection of neurons, typically in the form of a thin surface. However, it usually refers to the cerebral cortex, the outermost layer of the cerebrum. It is 2.5 mm to 5 mm thick and rich in nerve cells. The cerebral cortex is heavily folded, comparable to a handkerchief in a cup. This creates numerous convolutions (gyri), fissures (fissurae), and sulci. Unfolded, the surface area of the cortex is approximately 1,800cm².
Prefrontal cortex
Prefrontal cortex
The prefrontal cortex (PFC) forms the front part of the frontal lobe and is one of the brain's most important integration and control centers. It receives highly processed information from many other areas of the cortex and is responsible for planning, controlling, and flexibly adapting one's own behavior. Its central tasks include executive functions, working memory, emotion regulation, and decision-making. In addition, the PFC plays an important role in the cognitive evaluation and modulation of pain.





Mysterious patient
However, it is not only injury to the ARAS that can drastically impair Perception. In 2009, a medical case report was published about a young man from Mexico City who initially puzzled the emergency services. The 27-year-old was alert and conscious but appeared to be frozen. He moved in response to pain stimuli, but did not respond to speech, as described in the British Journal of Medical Case Reports.
What had happened? Imaging revealed that the patient had suffered a particularly severe infarction in the thalamus. This region of his brain had almost completely failed. The thalamus is not called “the gateway to consciousness” for nothing: “This is where the nerve pathways of all the sensory organs are switched before they are forwarded to the cerebral cortex,” explains Singer, “so this core area decides which sensory stimuli actually reach the cerebrum.” (For the exception of “smell,” see the box “Smell awakens memories.”)
Every spoken word and every flash of light first passes through the thalamus before we even become aware of it. Accordingly, the rescue workers' questions could hardly penetrate the young man's consciousness. Since his thalamus was no longer functioning properly, the neural signals were stopped here before they could reach the cerebral Cortex and thus his consciousness. Only very strong stimuli, such as pain, could pass through the defective core area.
Perception
The term describes the complex process of gathering and processing information from stimuli in the environment and from the internal states of a living being. The brain combines the information, which is perceived partly consciously and partly unconsciously, into a subjectively meaningful overall impression. If the data it receives from the sensory organs is insufficient for this, it supplements it with empirical values. This can lead to misinterpretations and explains why we succumb to optical illusions or fall for magic tricks.
Cortex
cortex cerebri
Cortex refers to a collection of neurons, typically in the form of a thin surface. However, it usually refers to the cerebral cortex, the outermost layer of the cerebrum. It is 2.5 mm to 5 mm thick and rich in nerve cells. The cerebral cortex is heavily folded, comparable to a handkerchief in a cup. This creates numerous convolutions (gyri), fissures (fissurae), and sulci. Unfolded, the surface area of the cortex is approximately 1,800cm².
Halved perception
If, on the other hand, the dysfunction affects downstream brain regions, Attention is only limited within certain areas. Neglect, for example, shows the consequences that the failure of one Hemisphere can have. The term is derived from the Latin word “neglegere,” which means “not knowing” or “neglecting.” Because that is exactly what happens with Neglect: half of the environment is ignored.
Neglect usually occurs as a result of a stroke in the right posterior cerebral Cortex. However, since sensory information crosses this side on its way to the brain, the perceptual disorder affects the opposite side: everything that happens on the left no longer enters consciousness, while everything that happens on the right is perceived normally. This results in bizarre situations in everyday life that the patient himself does not notice: he only shaves the right side of his face, or only eats the food on the right side of his plate. The left side, on the other hand, is ignored: the vegetables remain untouched and the stubble continues to grow. The same applies to additional unilateral lesions of the Basal ganglia for motor function. Here, too, one side is completely neglected: the left leg and left arm are hardly moved, even though they are functionally capable; their existence is ignored.
Attention
Attention
Attention serves as a tool for consciously perceiving internal and external stimuli. We achieve this by focusing our mental resources on a limited number of stimuli or pieces of information. While some stimuli automatically attract our attention, we can select others in a controlled manner. The brain also unconsciously processes stimuli that are not currently the focus of our attention.
Hemisphere
The cerebrum and cerebellum each consist of two halves – the right and left hemispheres. In the cerebrum, they are connected by three pathways (commissures). The largest commissure is the corpus callosum.
Neglect
Neglect is a perceptual disorder in which parts of the body or stimuli are ignored due to a brain lesion. The disorder affects the sides opposite the brain lesion. It usually occurs after lesions in the right parietal lobe. Accordingly, visual, auditory, and somatosensory stimuli on the left side are ignored.
stroke
Cerebral apoplexy
In a stroke, the brain or parts of it are no longer supplied with sufficient blood, which impairs the supply of oxygen and glucose. The most common cause is a blockage in an artery (ischemic stroke), less commonly a hemorrhage (hemorrhagic stroke). Typical symptoms include sudden visual disturbances, dizziness, paralysis, speech or sensory disturbances. Long-term consequences can include various sensory, motor, and cognitive impairments.
posterior
A positional term – posterior means "towards the back, located at the rear." In relation to the nervous system, it refers to a direction towards the tail.
Cortex
cortex cerebri
Cortex refers to a collection of neurons, typically in the form of a thin surface. However, it usually refers to the cerebral cortex, the outermost layer of the cerebrum. It is 2.5 mm to 5 mm thick and rich in nerve cells. The cerebral cortex is heavily folded, comparable to a handkerchief in a cup. This creates numerous convolutions (gyri), fissures (fissurae), and sulci. Unfolded, the surface area of the cortex is approximately 1,800cm².
Basal ganglia
Nuclei basales
The basal ganglia are a group of subcortical nuclei (located beneath the cerebral cortex) in the telencephalon. The basal ganglia include the globus pallidus and the striatum, and, depending on the author, other structures such as the substantia nigra and the subthalamic nucleus. The basal ganglia are primarily associated with voluntary motor function, but they also influence motivation, learning, and emotion.
Further reading:
- Lopez-Serna R et al.: Bilateral thalamic stroke due to occlusion of the artery of Percheron in a patient with patent foramen ovale: a case report. J Med Case Rep. 2009 Sep 15;3:7392. doi: 10.4076÷1752−1947−3−7392 (to the text).
stroke
Cerebral apoplexy
In a stroke, the brain or parts of it are no longer supplied with sufficient blood, which impairs the supply of oxygen and glucose. The most common cause is a blockage in an artery (ischemic stroke), less commonly a hemorrhage (hemorrhagic stroke). Typical symptoms include sudden visual disturbances, dizziness, paralysis, speech or sensory disturbances. Long-term consequences can include various sensory, motor, and cognitive impairments.
First published on August 27, 2013
Last updated on June 13, 2025